ACUTE CHILDHOOD LEUKEMIA
By Sandy Effendi,
a staff nurse mubarak al kabeer hospital
A progressive, malignant disease of the blood-forming tissues that is characterized by the uncontrolled proliferation of immature leukocytes and their precursors, particularly in the bone marrow, spleen, and lymph nodes. It is the most frequent cancer in the children, with a peak onset occurring between 2 and 5 years of age.
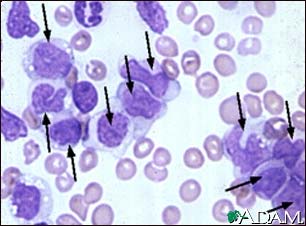
> OBSERVATIONS: Acute leukemia is classified according to cell type: acute lymphoid leukemia (ALL) includes lymphatic, lymphocytic. Lymphoblastic, and lymphoblastoid types; acute nonlymphoid leukemia (ANLL) includes granulocytic, myelocytic, monocytic, myelogeneous, monoblastic, and monomyeloblastic types (the myelocytic and monocytic series are abbreviated AML). ALL is predominantly a disease of childhood, whereas AML occurs in all age groups. The traditional classification of leukemia into chronic and acute types is based on duration or expected course of illness and the relative maturity of the leukemic cells. Although this classification is still used, particularly to chronic, forms of disease, it is no longer valid as a prognostic indication. The exact cause of the disease is unknown, although various factors are implicated, including genetic defects, immune deficiency, viruses, and carcinogenic environmental factors, primarily ionizing radiation. In acute leukemia, large immature leukocytes accumulate rapidly and infiltrate other tissues of the body, especially the reticuloendothelial system, causing decreased production of erythrocytes and platelets. Neutropenia, anemia, and increased susceptibility to infection and hemorrhage, and weakening of the bones with tendency to fracture also occur. Initial symptoms of the disease include fever, pallor, fatigue, anorexia, secondary infections (usually of the mouth, throat, or lungs), bone and join pain, subdermal or submucosal hemorrhage, and enlargement of the spleen, liver, and lymph nodes. Onset may be abrupt or follow a gradual, progressive course. Involvement of the central nervous system may lead to leukemic meningitis. Characteristically, a peripheral blood smear reveals many immature leukocytes. The diagnosis is confirmed by bone marrow aspiration or biopsy and examination, which show a highly elevated number of lymphoblast with almost complete absence of erythrocytes, granulocytes and megakaryocytes. The prognosis is poor and untreated cases, and death occurs usually within 6 months after the onset of symptoms. Survival rates have dramatically increased in recent years with the use of antileukemic agents in combination regimens. Remission of 5 years or longer occurs in 50 % to 70% of children with ALL, with 20% to 30% achieving complete remission. For children with AML, the prognosis is poorer, and remission rate is far less.
> INTERVENTION: Treatment of acute leukemia consists of three-stage process involving the use of chemotherapeutic agents and irradiation. In the first, or remission induction, phase complete destruction of all leukemic cells is achieved within a 4-to 6 week period using a combination drug-therapy regimen. The main drugs used in ALL are the corticosteroids, usually three daily oral doses of prednisone; vincristine, administered intravenously once a week; and 1-asparaginase, given intramuscularly three times a week for a total of nine doses. Allopurinol, a xanthine-oxidase inhibitor, is usually administered to inhibit uric acid production. Other drugs used in various combination regimens in sequential cycles include methotrexate, 6-mercaptopurine, cyclophospamide, cytosine arabiniside, hydroxyurea, daunorubicin, and doxorubicin. In children with AML the primary drugs of induction remission are 6-thioguanine, daunomycin, cytosine arabinoside, 5-azacytidine, vincristine, and prednisone. The child is usually hospitalized for part or all of the treatment because of the many side effects of the drugs and the high risk of complications, especially infection and hemorrhage. If severe hemorrhaging occurs and does not respond to local treatment, platelet transfusions may be necessary, and in cases of severe anemia, especially during induction therapy. Whole blood or packed red cells may be needed to raise hemoglobin levels. The second stage of treatment involves prophylactic maintenance to prevent leukemic infiltration of the central venous system. Because chemotherapy drugs do not cross the blood-brain barrier, therapy usually consists of daily high-dose of cranial irradiation for about two weeks after induction remission and weekly or twice-weekly doses of intrathecal methotrexate, for a total of five or six injections, although in some cases only the drug is given, In small children the irradiation is limited to the cranium to prevent retardation of linear growth, but older children may receive craniospinal radiation. Therapy of maintain remission usually begins after the child is discharge from the hospital and consists of various regimens of drugs in combination. A common schedule includes daily oral doses of 6-mercaptopurine and weekly doses of oral methotrexate, intermittent short-term therapy with prednisone an vincristine, and periodic doses of intrathecal methotrexate for prophylaxis against spread to the central nervous system. Complete blood counts are done weekly or monthly, and bone marrow examinations are performed every 3 to 4 months to detect myelosuppression and drug toxicity. Maintenance therapy is discontinued after a period of 2 to 3 years if initial remission is maintained. Continuous treatment beyond 3 years is not advised, as the adverse affects of the medications increase with prolonged use. Relapse occurs, the child begin treatment cycle again, usually with predisone, vincristine, and a combination of other drugs not previously tried. With each relapse the prognosis becomes poorer. Other treatments for prolonging remission include immunotherapy using periodic inoculation with BCG vaccine or bone marrow transplant, which has been successful in including long-term remissions in about 10% to 20% of the cases, especially those with AML or severe, terminal ALL.
> NURSING CONSIDERATIONS: Nursing care for the child with acute leukemia involves intensive physical and emotional support during all phases of the disease, its diagnosis, and treatment. Foremost is the preparation of the child and parents for the various diagnostic and therapeutic procedures, including venipuncture, bone-marrow aspiration or biopsy, lumbar puncture, and x-ray treatment. Specific medical and nursing management depends on the particular regimen of drug therapy, although most of the chemotherapeutic agents used in treatment cause myelosuppression that may lead to secondary complications of infection, hemorrhage, and anemia. Overwhelming infection is a major problem and one of the most frequent causes of death. Severe neutropenia indicate increased risk of infection. It may occur during immunosuppressive therapy or after prolonged antibiotic therapy. The most common infectious organisms are viruses, especially varicella, herpes zoster, herpes simplex, measles, mumps, rubella, and poliomyelitis, both gram positive and gram-negative bacteria, including Staphylococcus aureus, S. epidermidis, group-A beta-hemolytic Streptococcus, Pseudomonas aeruginosa, Escerichia coli, Proteus, and klebsiella, and various parasites and fungi, especially pneumocytis carinii and candida albicans. To prevent infection, the nurse isolates the child as much as possible, screens visitors for active infection, institutes strict aseptic procedures, monitors temperature closely, evaluates possible sites of infection (such as needle punctures), encourage adequate nutrition, helps the child to avoid exertion or fatigue, and, at discharge, teaches the child and parents the necessity for voiding all known sources of infection. Primarily the common childhood communicable disease. Preventive measures to control infection also help decrease the tendency toward hemorrhage. Special attention is given to skin care, oral hygiene, cleanliness of the perineal area, and restriction of activities that could result in accidental injury. A major nursing consideration is the management of the many side effects resulting from drug toxicity and irradiation, including weakness and numbing of the extremities and severe jaw pain. Although corticosteroid treatment usually increase the appetite and produces a euphoric sense of well-being in the child, it also cause moon face, which is reversed with cessation of the steroid therapy. During maintenance therapy, the nurse continues to provide emotional support and guidance, specifically teaching parents which side effects are normal reactions to drugs and which indicate toxicity and require medical attention. In terminal stages of the disease, relief of discomfort and pain become primary focus. Effective measures include careful physical handling of the child, frequent position changes, avoidance of pressure on painful areas, and control of annoying environmental factors, such as excessive light and noise. Nonsalicylate analgesics are used as needed, depending on the severity of pain.
Source Mosby’s Dictionary 3rd edition
src="http://pagead2.googlesyndication.com/pagead/show_ads.js">
posted by Sandi at
10:08 PM
![]()

0 Comments:
Post a Comment
Subscribe to Post Comments [Atom]
<< Home